Systemic Conditions
Visceral Referral
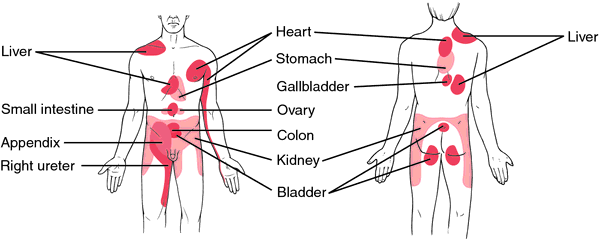
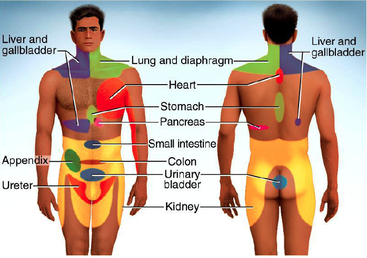
Referred pain from viscera can manifest from pathologic conditions such as ureteral colic or myocardial infarction and in non-pathologic conditions such as bowel and bladder distention. The pain can be referred from the viscera to the skin, muscle or regionally which may involve skin and muscle. The figure represents common referral patterns from visceral pain (notice the large areas colored around the shoulder girdle). While if only lung, diaphragm, liver and gallbladder are listed specifically for the shoulder area, it is important to note many organs including the stomach, intestines, and spleen can irritate the diaphragm and result in referred pain to the left shoulder. Kehr’s sign commonly refers to acute pain in the left shoulder due to the presence of a diaphragmatic irritant, ruptured spleen or ruptured ectopic pregnancy. Pain will also be felt in the abdomen if pressure is applied to the upper left quadrant which can serve as a quick screen to help rule out visceral involvement. Murphy’s percussion test (shown in the video on home page) is a quick screen for renal system involvement where a percussive pressure is applied to the costovertebral angle. If pain is reported it is a yellow flag of kidney involvement that needs to be referred for further investigation.
Visceral referred pain shares the same central mechanisms as pain input from other structures that may lead to hypersensitivity, allodynia and expansion of receptive fields. Tissue damage is not necessary to produce visceral pain; it may be caused by non-damaging mechanisms such as distention, abnormal contraction, or traction. However, there are common damaging mechanisms that due cause shoulder pain. It should be questioned if meals effect the pain. If it occurs immediately after a meal it may indicate visceral involvement. If the shoulder pain is worsening a few hours after taking NSAIDs, it may indicate gastrointestinal ulcers especially if the patient has a previous history of ulcers.
Due to viscerosomatic convergence referred pain occurs, nearly all dorsal horn cells driven by visceral input have additional somatic input that the central nervous system (CNS) does not differentiate past the point. For example the diaphragm, the phrenic nerve that innervates the diaphragm is derived from C3-C5, which also extends to the upper shoulder region around the C4-C5 distribution. The key to differentiating the pain comes from the patient’s description of the pain. A deep dull aching pain that is relatively static, localized, and not heavily influenced by movement often characterizes visceral pain. If the shoulder pain is accompanied by a persistent cough, blood speckled sputum, deep inspiration, chest pain, nausea, vomiting, jaundice or pain with laying down or laughing there is likely a serious visceral illness involved. It is also important to question the patient about other pain they may be feeling and does eating alter the symptoms. Similar to musculoskeletal pain presentation the patient may find a position that relieves their pain, for example leaning towards the affected kidney may reduce symptoms, and leaning forward may ease pain gallbladder and pancreas pain. Screening for medical disease and continual monitoring for unexpected patient responses to physical therapy intervention along with a thorough history, physical examination and some degree of suspicion are required to ensure the identification of conditions that are not truly musculoskeletal in nature.
Visceral referred pain shares the same central mechanisms as pain input from other structures that may lead to hypersensitivity, allodynia and expansion of receptive fields. Tissue damage is not necessary to produce visceral pain; it may be caused by non-damaging mechanisms such as distention, abnormal contraction, or traction. However, there are common damaging mechanisms that due cause shoulder pain. It should be questioned if meals effect the pain. If it occurs immediately after a meal it may indicate visceral involvement. If the shoulder pain is worsening a few hours after taking NSAIDs, it may indicate gastrointestinal ulcers especially if the patient has a previous history of ulcers.
Due to viscerosomatic convergence referred pain occurs, nearly all dorsal horn cells driven by visceral input have additional somatic input that the central nervous system (CNS) does not differentiate past the point. For example the diaphragm, the phrenic nerve that innervates the diaphragm is derived from C3-C5, which also extends to the upper shoulder region around the C4-C5 distribution. The key to differentiating the pain comes from the patient’s description of the pain. A deep dull aching pain that is relatively static, localized, and not heavily influenced by movement often characterizes visceral pain. If the shoulder pain is accompanied by a persistent cough, blood speckled sputum, deep inspiration, chest pain, nausea, vomiting, jaundice or pain with laying down or laughing there is likely a serious visceral illness involved. It is also important to question the patient about other pain they may be feeling and does eating alter the symptoms. Similar to musculoskeletal pain presentation the patient may find a position that relieves their pain, for example leaning towards the affected kidney may reduce symptoms, and leaning forward may ease pain gallbladder and pancreas pain. Screening for medical disease and continual monitoring for unexpected patient responses to physical therapy intervention along with a thorough history, physical examination and some degree of suspicion are required to ensure the identification of conditions that are not truly musculoskeletal in nature.
References
Fruth, S. J. (2006). Differential diagnosis and treatment in a patient with posterior upper thoracic pain. Phys Ther, 86(2), 254-268.
Gerwin, R. D. (2002). Myofascial and visceral pain syndromes: visceral-somatic pain representations... The Fifth World Congress on Myofascial Pain and Fibromyalgia, MYOPAIN 2001, Portland, Oregon, USA, September 9-13, 2001. Journal of Musculoskeletal Pain, 10(1/2), 165-175.
Horsley, I. (2010). Is It Really A Shoulder Problem? A Differential diagnosis of shoulder pain. SportEX Dynamics(24), 20-23.
Soyuncu, S., Bektas, F., & Cete, Y. (2012). Traditional Kehr's sign: Left shoulder pain related to splenic abscess. Ulus Travma Acil Cerrahi Derg, 18(1), 87-88.
Stopka, C. B., & Zambito, K. L. (1999). Referred Visceral Pain: What Every Sports Medicine Professional Needs to Know. Athletic Therapy Today, 4(1), 29-36.
Gerwin, R. D. (2002). Myofascial and visceral pain syndromes: visceral-somatic pain representations... The Fifth World Congress on Myofascial Pain and Fibromyalgia, MYOPAIN 2001, Portland, Oregon, USA, September 9-13, 2001. Journal of Musculoskeletal Pain, 10(1/2), 165-175.
Horsley, I. (2010). Is It Really A Shoulder Problem? A Differential diagnosis of shoulder pain. SportEX Dynamics(24), 20-23.
Soyuncu, S., Bektas, F., & Cete, Y. (2012). Traditional Kehr's sign: Left shoulder pain related to splenic abscess. Ulus Travma Acil Cerrahi Derg, 18(1), 87-88.
Stopka, C. B., & Zambito, K. L. (1999). Referred Visceral Pain: What Every Sports Medicine Professional Needs to Know. Athletic Therapy Today, 4(1), 29-36.
A.T. Still University
Class of 2015
Published 07/03/2014
Class of 2015
Published 07/03/2014
