Cloward's Areas
According to Cloward (1959), pain in the neck, shoulder, and arm is an essential part of syndromes involving a ruptured cervical disk. Patients often complain of pain located in the region of the shoulder blade, which in the 1950’s was a mysterious phenomenon. Multiple studies involving patients with cervical dysfunction complained of scapula pain and also increased irritability of local muscles in the tender areas. Despite the fact that the skin of the scapulothoracic area is innervated by the 2nd to 7th thoracic nerve roots, the nerve innervation for the muscles beneath originate from the brachial plexus of the cervical areas. This fact has lead to the hypothesis that scapular pain due to lower cervical disk lesions may have motor contributions. The innervations are as follows:
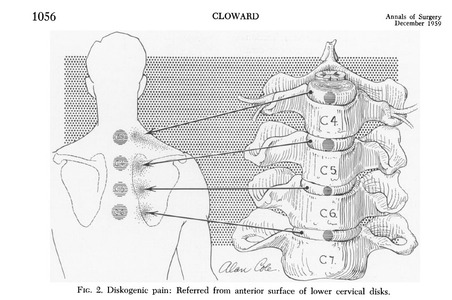
When examining pain in the scapular region it is often referred to as a deep, dull ache. The image illustrates the cervical referral pattern into the scapulothoracic region. Much research has taken place in order to identify referral patterns and to create a “symptom map” of sorts. Research has found that the C2–C3 disc refers pain to the neck, subocciput and face. The C3–C4 disc refers pain to the neck, subocciput, trapezius, anterior neck, face, shoulder, interscapular and limb. The C4–C5 disc refers pain to the neck, shoulder, interscapular, trapezius, extremity, face, chest and subocciput. The C5–C6 disc refers pain to the neck, trapezius, interscapular, suboccipital, anterior neck, chest and face. The C6–C7 disc refers pain to the neck, interscapular, trapezius, shoulder, extremity and subocciput. Lastly, for C7–T1 neck and interscapular pain is often reproduced. This is consistent with but also expands on Cloward's areas of referral. The common variable of cervical disc dysfunction is the direct involvement of the scapulothoracic region, making neck screens a crucial aspect of the Physical Therapy exam when a patient complains of neck, shoulder, or scapular pain.
As with every musculoskeletal conditions, a thorough exam must be completed in order to identify the source of symptoms. This section highlights the fact that patient presentation is not always as it appears and further investigation is necessary in order to solve the mystery of their pain source. Scapulothoracic pain, as discussed above and in other sections of this website, may be attributed to skeletal, muscular, sensory, or visceral impairments.
- Levator Scapulae C3-C4
- Rhomboids C5
- Supra and infraspinatus muscles C5-C6
- Subscapularis C6-C7
- Latissimus Dorsi C6-C7
When examining pain in the scapular region it is often referred to as a deep, dull ache. The image illustrates the cervical referral pattern into the scapulothoracic region. Much research has taken place in order to identify referral patterns and to create a “symptom map” of sorts. Research has found that the C2–C3 disc refers pain to the neck, subocciput and face. The C3–C4 disc refers pain to the neck, subocciput, trapezius, anterior neck, face, shoulder, interscapular and limb. The C4–C5 disc refers pain to the neck, shoulder, interscapular, trapezius, extremity, face, chest and subocciput. The C5–C6 disc refers pain to the neck, trapezius, interscapular, suboccipital, anterior neck, chest and face. The C6–C7 disc refers pain to the neck, interscapular, trapezius, shoulder, extremity and subocciput. Lastly, for C7–T1 neck and interscapular pain is often reproduced. This is consistent with but also expands on Cloward's areas of referral. The common variable of cervical disc dysfunction is the direct involvement of the scapulothoracic region, making neck screens a crucial aspect of the Physical Therapy exam when a patient complains of neck, shoulder, or scapular pain.
As with every musculoskeletal conditions, a thorough exam must be completed in order to identify the source of symptoms. This section highlights the fact that patient presentation is not always as it appears and further investigation is necessary in order to solve the mystery of their pain source. Scapulothoracic pain, as discussed above and in other sections of this website, may be attributed to skeletal, muscular, sensory, or visceral impairments.
References
Cloward, Howard (1959). Cervical diskography: contribution to the etiology and mechanism of neck, shoulder, and arm pain. Annals of Surgery 150 (6), 1052-1064.
Slipman, Curtis, Plastaras, Chris, Patel, Rajeev, Isaac, Zacharia, Chow, David, Garvan, Cynthia, Pauza, Kevin, & Furman, Michael (2005). Provocative cervical discography symptom mapping. The Spine Journal 5, 381–388.
Slipman, Curtis, Plastaras, Chris, Patel, Rajeev, Isaac, Zacharia, Chow, David, Garvan, Cynthia, Pauza, Kevin, & Furman, Michael (2005). Provocative cervical discography symptom mapping. The Spine Journal 5, 381–388.
A.T. Still University
Class of 2015
Published 07/03/2014
Class of 2015
Published 07/03/2014
