Neurological Conditions
Brachial Plexus
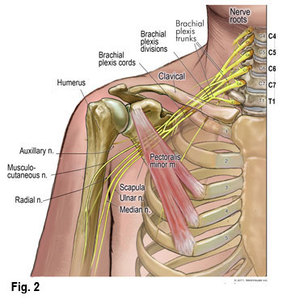
Anatomy Description: The brachial plexus is a network of nerves supplying the upper limb and shoulder girdle, arising from spinal roots C5 to T1. The spinal roots of C5 to T1 merge to form three trunks: superior (C5-6), middle (C7), and inferior (C8-T1). The brachial plexus is located in the neck. The trunks of the brachial plexus lie in the posterior triangle of the neck, covered by skin, platysma, and deep fascia. Additionally, the brachial plexus roots lie between the anterior and middle scalene muscles. The divisions of the brachial plexus lie behind the clavicle and the cords in the axillary region. The branches of the brachial plexus, which arise from the roots or trunks or cords, are located supraclavicular or infraclavicular.
Epidemiology: Brachial plexus injury (BPI) is a common injury that leads to loss of sensation, motor control, and many experience disabling neuropathic pain. The prevalence of BPIs in adults is approximately 1.2% of the total trauma population. BPIs usually affect young healthy male adults (89%). The age of patients ranges between 14 to 63 years, with a mean of 29 years and a median of 25 years of age. Fifty percent of patients are between 19 and 34 years old. Between 44% and 70% of BPI are caused by traumatic injuries, mostly occurring in motorcycle accidents, during sporting activities, at the workplace, or during surgical or anesthetic procedures.
Mechanism of Injury: Traumatic injuries results in traction forces where the arm and shoulder are forcefully distracted away from the neck or trunk, crush, or compression cause by various mechanisms, such as compression of the clavicle against the rib cage due to seatbelt restraint, anterior shoulder dislocation, tumors, inflammatory diseases, stab and gun shot wounds, radiation, Parsonage-Turner Syndrome, or surgical positioning.
Features:
Diagnosing:
Physical Therapy Management:
Medical Management:
Prognosis:
Differential Diagnosis:
Epidemiology: Brachial plexus injury (BPI) is a common injury that leads to loss of sensation, motor control, and many experience disabling neuropathic pain. The prevalence of BPIs in adults is approximately 1.2% of the total trauma population. BPIs usually affect young healthy male adults (89%). The age of patients ranges between 14 to 63 years, with a mean of 29 years and a median of 25 years of age. Fifty percent of patients are between 19 and 34 years old. Between 44% and 70% of BPI are caused by traumatic injuries, mostly occurring in motorcycle accidents, during sporting activities, at the workplace, or during surgical or anesthetic procedures.
Mechanism of Injury: Traumatic injuries results in traction forces where the arm and shoulder are forcefully distracted away from the neck or trunk, crush, or compression cause by various mechanisms, such as compression of the clavicle against the rib cage due to seatbelt restraint, anterior shoulder dislocation, tumors, inflammatory diseases, stab and gun shot wounds, radiation, Parsonage-Turner Syndrome, or surgical positioning.
Features:
- Pain is most common, in particular those affecting the preganglionic fibers. Often described as crushing with intermittent severe attacks shooting down the arm.
- Paralysis and anaesthesia in affected extremity
- Bizarre sensations, hyperalgesia, dysesthesia and allodynia
- Myoclonic jerks in the affected extremity
- Ipsilateral Horner's Syndrome with sympathetic ganglion (T1) injury
- Winged Scapula with long thoracic nerve (C5-C7) injury
- Atrophy of parascapular muscles with dorsal scapular (C4-C7) injury
- Cervical paraspinal muscle weakness and loss of posterior neck sensation with dorsal rami of cervical spinal nerve roots injury
- Hemidiaphragm paralysis with phrenic nerve (C3-C5) injury
- Possible motor deficits in C5-T1 nerve roots based on injury
Diagnosing:
- The patient’s history is essential in identification of the traumatic mechanism of injury, associated injuries, and previous treatment
- The character and severity of pain should be documented
- Motor and sensory examination of the injured limb and a global neurologic examination should be done since associated cervical spine and spinal cord injury are not uncommon
- A focused examination of the injured limb should be performed, including an assessment of the functional deficits
- The motor control/strength of every muscle should be documented
- Skin bruising and focal ecchymosis can be observed
- Currently computed tomography-myelography (CT-myelography) is considered the gold standard to identify the site of lesions and the amount of damage
- Radiographs are used to detect fractures, dislocation of ribs, shoulder girdle depression, hemidiaphragm elevation (phrenic nerve palsy), and dislocation of the scapula.
- Angiography is suggested to rule out major vessel injury associated with BPI. The vessels most often damaged include subclavian artery, subclavian vein, and the axillary artery
Physical Therapy Management:
- The main goals in the rehabilitation of BPIs are prevention of muscle atrophy, prevention and restraint of secondary deformities, pain suppression, recovery of somatosensory deficits, learned non-use, and postoperative care.
- Treatment approaches to fulfill main goals in rehabilitation (based on evidence) could include:
- Rehabilitation approach aimed at returning the patient back to work and recreation as soon as possible is effective in distracting patients from pain
- Passive muscle stretching & strengthening
- Use of orthoses/splints
- Transcutaneous electrical nerve stimulation (TENS) applied to painful areas
- Electrical stimulation applied to the injured nerve or the denervated muscle
- Laser therapy
- Ultrasound
- Acupuncture
- Exercises retraining of tactile gnosis using different shapes and textures
- Mirror therapy
- Constrained Induced Movement Therapy (CIMT)
- Patient’s keep wearing the brace 6-8 weeks and then use a sling
- Passive stretching in external rotation should be performed to prevent secondary deformities and in particular to correct imbalance between strong internal rotation muscles and weak external rotators
Medical Management:
- The main aspect of medical management is pain control. They often treat this pain similar to neuropathic pain
- Surgical interventions include nerve transfer surgery and use of functioning free muscle transfers or nerve transfers may restore hand function, with variable results.
Prognosis:
- Early diagnosis is important since secondary damage could lead to disability and functional impairment
- It is difficult to predict or estimate the rate of recovery. The potential for recovery depends on the type and severity of injury. As a result, the prognosis must be assessed for each patient individually based on the type and severity of their injury, and the progression of any recovery that may be occurring.
Differential Diagnosis:
- Sepsis with localization at the glenohumeral joint
- Acromioclavicular Joint Injury
- Cervical Disc Injuries
- Cervical Discogenic Pain Syndrome
- Cervical Radiculopathy
- Cervical Spine Sprain/Strain Injuries
- Shoulder Dislocation
- Shoulder Impingement Syndrome
- Thoracic Outlet Syndrome
Brachial Plexus References
Limthongthang, R., Bachoura, A., Songcharoen, P., & Osterman, AL. (2013). Adult Brachial Plexus Injury: Evaluation and Management. Orthop Clin North Am. Oct; 44(4): 591-603. doi: 10.1016/j.ocl.2013.06.011.
Monteiro, M.J., Altman, K., & Khandwala, A. 2010. Injury to the brachial plexus in neck dissections. British Journal of Oral and Maxillofacial Surgery. 04-01, Volume 48, Issue 3, Pages 197-19.
Shveiky, D., Aseff, N.J., & Iglesia, B.C. 2010. Brachial Plexus Injury after Laparoscopic and Robotic Surgery. Journal of Minimally Invasive Gynecology, The Journal of Minimally Invasive Gynecology. 07-01, Volume 17, Issue 4, Pages 414-420
Smania, N., Berto, G., La Marchina, E., Melotti, C., Midiri, A., Roncari, L., Zenorini, A., Ianes, P., Picelli, A., Waldner, A., Faccioli, S., & Gandolfi, M. (2012). Eur J Phy Rehabil Med. Sep; 48 (3): 483-506
Monteiro, M.J., Altman, K., & Khandwala, A. 2010. Injury to the brachial plexus in neck dissections. British Journal of Oral and Maxillofacial Surgery. 04-01, Volume 48, Issue 3, Pages 197-19.
Shveiky, D., Aseff, N.J., & Iglesia, B.C. 2010. Brachial Plexus Injury after Laparoscopic and Robotic Surgery. Journal of Minimally Invasive Gynecology, The Journal of Minimally Invasive Gynecology. 07-01, Volume 17, Issue 4, Pages 414-420
Smania, N., Berto, G., La Marchina, E., Melotti, C., Midiri, A., Roncari, L., Zenorini, A., Ianes, P., Picelli, A., Waldner, A., Faccioli, S., & Gandolfi, M. (2012). Eur J Phy Rehabil Med. Sep; 48 (3): 483-506
Thoracic Outlet Syndrome
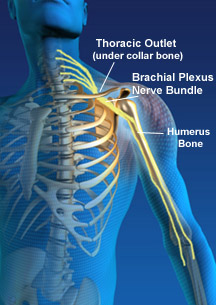
Description: Thoracic outlet syndrome (TOS) is due to peripheral nerve compression. The term thoracic outlet syndrome was originally coined in 1956 by Peet to indicate compression of the neurovascular structures in the interscalene triangle. TOS encompasses a wide range of clinical manifestations due to compression of nerves and vessels during their passage through the neural container. The overall incidence of TOS is estimated at over 90% of all TOS cases are of neurogenic origin, whereas less than 1% are arterial and approximately 3-5% are venous. Neurogenic TOS are classified as either true neurogenic or disputed neurogenic. True Neurogenic is associated with neurological deficits due to muscular atrophy, whereas disputed neurogenic is not associated with objective neurological deficits.
Anatomy Review: The neural container described as the thoracic outlet is comprised of several structures, and is divided into two main sections by the first rib. The proximal portion consists of the interscalene triangle, which is the 1st and most proximal passageway-this triangle is bordered by the anterior scalene muscle anteriorly, the middle scalene muscle posteriorly, and the medial surface of the first rib inferiorly. The brachial plexus and the subclavian artery pass through this space. The costoclavicular space, which is the 2nd passageway and is bordered anteriorly by the middle third of the clavicle, posteromedially by the first rib, and posterolaterally by the upper border of the scapula. The neurovascular bundle enters into this space. The last passageway called the thoraco-coraco-pectoral space include the coracoid process superiorly, the pectoralis minor anteriorly, and the ribs 2 through 4 posteriorly. The axilla or axillary region comprises the distal aspect of the canal. However, the proximal portion has more clinical relevance since there is a higher potential for neurovascular compression at that site. Additionally, there are several types of anatomical abnormalities that exist and produce the compromising events related to TOS, which include the presence of a cervical rib, congenital soft tissue abnormalities, clavicular hypomobility, and functionally acquired anatomical changes.
Incidence: TOS is typically diagnosed between the ages of 20 to 50 years. Women are three to four time more likely to develop neurogenic TOS. The incidence of vascular TOS is equal between non-athletic men and women; however, it is found to be greater in competitive athletic men versus women.
Mechanism of Injury: Arterial TOS: often in young adults with a history of vigorous arm activity or spontaneous. Venous TOS: pain, in younger men and often proceeded by excessive activity in the arms or spontaneous edema of the arm. True Neurogenic TOS: history of neck trauma preceding symptoms, most commonly from car accidents and repetitive stress at work. Disputed TOS: Common history of neck trauma preceding the symptoms, most commonly from car accidents and repetitive stress at work.
Features: Arterial TOS: Pain in the hand but seldom in the shoulder and neck. Pallor. Claudication. Cold intolerance. Paresthesias: symptoms usually stem from arterial emboli. Venous TOS: Feeling of heaviness. Cyanosis. Paresthesias in the fingers and hand secondary to edema. True Neurogenic TOS: Pain, paresthesia, numbness and/or weakness in the hand, plus neck pain. Headaches. Paresthesias, numbness during the day and night and awakening with pain and numbness. Loss of dexterity. Objective weakness and/or sensory deficits. Cold Intolerance. Raynaud phenomenon. Disputed TOS: Pain, paresthesia, and feeling of weakness in the hand, arm (C8, T1 distribution) and shoulder, plus neck pain. Headaches. Often wake during night due to paresthesia or pain. Loss of dexterity. Cold intolerance. Raynaud phenomenon.
Diagnosing: This can be difficult since symptoms vary between patients due the location of nerve or vessel involvement. A careful history and thorough clinical examination are the most important components in establishing the diagnosis of TOS, which remains a diagnosis of exclusion. Arterial TOS: Confirmed through Doppler ultrasound and angiography in the seated position. Venous TOS: confirmed through venous ultrasound studies, venous scintillation scans, venography and plethysmography. True Neurogenic TOS: Based on information from a cluster of signs and symptoms and at least two provocation tests positive and almost always elevated arm stress test (+). Confirmed through neurophysiological tests (+). Disputed TOS: Based on information a cluster of signs and symptoms and at least two provocation tests positive and often presence of cyriax release test (+). No confirmation through neurophysiological tests since they are normal.
Differential Diagnosis:
Special Tests:
Medical and Surgical Management: Drug therapy that includes ibuprofen, tricyclic antidepressants, and anticonvulsants. In determining, the need for surgical therapy requires careful consideration. Caution is also necessary in patients with work-related injuries or where litigation may be a concern. Consider surgery if there is: wasting of muscles, vascular involvement, or loss of function. Also, consider surgery if, after several months, conservative treatment has failed. Surgical management of TOS may include a variety of approaches including supraclavicular decompression, transaxillary, resection of the clavicle, division of the scalenus anterior muscle, division of the pectoralis minor tendon, and excision of the first or cervical ribs, or a combination of one or more techniques.
Physical Therapy Management: It is shown in the literature that a conservative approach can resolve TOS is 60 percent of cases. However, surgical management can resolve a majority of those cases that fail with conservative therapy. The goals of physical therapy are to strengthen the shoulder girdle, improve posture, and prevent hyper-abduction. Specific therapeutic treatments can include based on literature:
Prognosis:
Anatomy Review: The neural container described as the thoracic outlet is comprised of several structures, and is divided into two main sections by the first rib. The proximal portion consists of the interscalene triangle, which is the 1st and most proximal passageway-this triangle is bordered by the anterior scalene muscle anteriorly, the middle scalene muscle posteriorly, and the medial surface of the first rib inferiorly. The brachial plexus and the subclavian artery pass through this space. The costoclavicular space, which is the 2nd passageway and is bordered anteriorly by the middle third of the clavicle, posteromedially by the first rib, and posterolaterally by the upper border of the scapula. The neurovascular bundle enters into this space. The last passageway called the thoraco-coraco-pectoral space include the coracoid process superiorly, the pectoralis minor anteriorly, and the ribs 2 through 4 posteriorly. The axilla or axillary region comprises the distal aspect of the canal. However, the proximal portion has more clinical relevance since there is a higher potential for neurovascular compression at that site. Additionally, there are several types of anatomical abnormalities that exist and produce the compromising events related to TOS, which include the presence of a cervical rib, congenital soft tissue abnormalities, clavicular hypomobility, and functionally acquired anatomical changes.
Incidence: TOS is typically diagnosed between the ages of 20 to 50 years. Women are three to four time more likely to develop neurogenic TOS. The incidence of vascular TOS is equal between non-athletic men and women; however, it is found to be greater in competitive athletic men versus women.
Mechanism of Injury: Arterial TOS: often in young adults with a history of vigorous arm activity or spontaneous. Venous TOS: pain, in younger men and often proceeded by excessive activity in the arms or spontaneous edema of the arm. True Neurogenic TOS: history of neck trauma preceding symptoms, most commonly from car accidents and repetitive stress at work. Disputed TOS: Common history of neck trauma preceding the symptoms, most commonly from car accidents and repetitive stress at work.
Features: Arterial TOS: Pain in the hand but seldom in the shoulder and neck. Pallor. Claudication. Cold intolerance. Paresthesias: symptoms usually stem from arterial emboli. Venous TOS: Feeling of heaviness. Cyanosis. Paresthesias in the fingers and hand secondary to edema. True Neurogenic TOS: Pain, paresthesia, numbness and/or weakness in the hand, plus neck pain. Headaches. Paresthesias, numbness during the day and night and awakening with pain and numbness. Loss of dexterity. Objective weakness and/or sensory deficits. Cold Intolerance. Raynaud phenomenon. Disputed TOS: Pain, paresthesia, and feeling of weakness in the hand, arm (C8, T1 distribution) and shoulder, plus neck pain. Headaches. Often wake during night due to paresthesia or pain. Loss of dexterity. Cold intolerance. Raynaud phenomenon.
Diagnosing: This can be difficult since symptoms vary between patients due the location of nerve or vessel involvement. A careful history and thorough clinical examination are the most important components in establishing the diagnosis of TOS, which remains a diagnosis of exclusion. Arterial TOS: Confirmed through Doppler ultrasound and angiography in the seated position. Venous TOS: confirmed through venous ultrasound studies, venous scintillation scans, venography and plethysmography. True Neurogenic TOS: Based on information from a cluster of signs and symptoms and at least two provocation tests positive and almost always elevated arm stress test (+). Confirmed through neurophysiological tests (+). Disputed TOS: Based on information a cluster of signs and symptoms and at least two provocation tests positive and often presence of cyriax release test (+). No confirmation through neurophysiological tests since they are normal.
Differential Diagnosis:
- Cervical disc herniation
- Cervical spondylosis
- Shoulder joint conditions: adhesive capsulitis, glenohumeral instability, glenohumeral or acromioclavicular osteoarthritis, rotator cuff tears, impingement, and bursitis
- Complex Regional Pain Syndrome
- Carpal tunnel syndrome
- Brachial plexus syndrome
- Ulnar nerve compression
- Multiple sclerosis
- Spinal cord and Pancoast tumors
- Raynaud phenomenon
Special Tests:
- Elevated Arm Stress
- Adson's
- Wright's
- Cyriax Release
- Supraclavicular Pressure
- Costoclavicular Maneuver
- Upper Limb Tension
- Cervical Rotation Lateral Flexion
Medical and Surgical Management: Drug therapy that includes ibuprofen, tricyclic antidepressants, and anticonvulsants. In determining, the need for surgical therapy requires careful consideration. Caution is also necessary in patients with work-related injuries or where litigation may be a concern. Consider surgery if there is: wasting of muscles, vascular involvement, or loss of function. Also, consider surgery if, after several months, conservative treatment has failed. Surgical management of TOS may include a variety of approaches including supraclavicular decompression, transaxillary, resection of the clavicle, division of the scalenus anterior muscle, division of the pectoralis minor tendon, and excision of the first or cervical ribs, or a combination of one or more techniques.
Physical Therapy Management: It is shown in the literature that a conservative approach can resolve TOS is 60 percent of cases. However, surgical management can resolve a majority of those cases that fail with conservative therapy. The goals of physical therapy are to strengthen the shoulder girdle, improve posture, and prevent hyper-abduction. Specific therapeutic treatments can include based on literature:
- Strengthen the trapezius muscles, rhomboids, levator scapulae, and rest of shoulder girdle
- Improve postural abnormalities
- Cervical traction for a short period of time
- Patient education: quit provoking behaviors, workplace ergonomics/posture
- Relaxation techniques
Prognosis:
- Prognosis is good for most patients with neurologic involvement who are treated with conservative management alone
- Prognosis also appears to be good for those with vascular involvement who undergo conservative therapy and for those with more serious involvement who ultimately require surgical intervention
TOS References
Hopper, TL., Denton, J., McGalliard, MK., Brismee, JM., & Sizer Jr, PS. 2010. Thoracic Outlet Syndrome. A controversial clinical condition. Part 1: anatomy, and clinical examination/diagnosis. Journal of Manual and Manipulative Therapy. 18(2). DOI 10.1179/106698110X12640740712734
Nichols A. Diagnosis and Management of Thoracic Outlet Syndrome. Current Sports Medicine Reports (American College Of Sports Medicine) [serial online]. September 2009;8(5):240-249.
Watson, L. A., Pizzari, T., & Balster, S. (2009). Thoracic outlet syndrome part 1: clinical manifestations, differentiation and treatment pathways. [Review]. Man Ther, 14(6), 586-595. doi:10.1016/j.math.2009.08.007
Nichols A. Diagnosis and Management of Thoracic Outlet Syndrome. Current Sports Medicine Reports (American College Of Sports Medicine) [serial online]. September 2009;8(5):240-249.
Watson, L. A., Pizzari, T., & Balster, S. (2009). Thoracic outlet syndrome part 1: clinical manifestations, differentiation and treatment pathways. [Review]. Man Ther, 14(6), 586-595. doi:10.1016/j.math.2009.08.007
Complex Regional Pain Syndrome in Adults (CRPS)
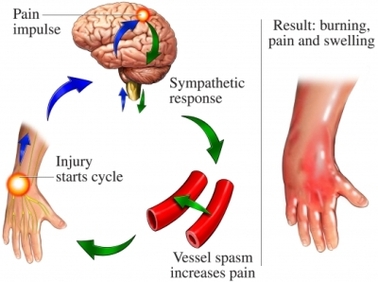
Description: Complex regional pain syndrome (CRPS) is a painful and debilitating condition in a limb that involves sensory, motor, autonomic, skin and bone abnormalities. There are two types of CRPS. CRPS type 1 involves no nerve injury, whereas, CRPS type 2 involves major nerve injury. Commonly, CRPS arises after an injury to that limb. However, there is no connection or relationship for the likelihood of developing CRPS based on the severity of trauma to that limb. In nine percent of cases, trauma is not a mechanism of injury in developing CRPS. CRPS commonly affects one limb, however, in seven percent of cases it later spreads to additional limbs. The incidence rate is 26/100,00 person-years. Research and clinical practice has found that this condition is not associated with a history of pain preceding psychological disorders, with somatization, or malingering. The primary cause of CRPS is unknown. The onsets of symptoms occur within one month of trauma, surgery, or immobilization. There is a not a cure for CRPS. Approximately 15% of patients with CRPS have severe pain and physical impairment two years after developing CRPS and are considered to have a long-term condition, however, more patients will have a lesser degree of ongoing pain and dysfunction. As a result, if a patient presents signs and symptoms of CRPS, they should be addressed with appropriate multidisciplinary medical services.
Features of CRPS:
Diagnostic Criteria: The diagnosis of CRPS is based on clinical examination and is given when patients meet the Budapest diagnostic criteria.
Budapest diagnostic criteria:
A) The patient has continuing pain which is disproportionate to any inciting event
B) The patient has at least one sign in tow or more of the categories
C) The patient reports at least one symptoms in three or more of the categories
D) No other diagnosis can be explain the signs and symptoms
Category
1. Sensory: Patients have signs and symptoms of Allodynia (to light touch and/or temperature sensation and/or deep somatic pressure and/or joint movement) and/or Hyperalgesia (to pinprick)
2. Vasomotor: Patients have signs and symptoms of temperature asymmetry (>1 degree Celsius) and/or skin color changes and/or skin color asymmetry.
3. Sudomotor/Edema: Patients have signs and symptoms of Oedema and/or sweating changes and/or swelling asymmetry
4. Motor/trophic: Patients have signs and symptoms of decreased range of motion and/or motor dysfunction (weakness, tremor, dystonia), and/or trophic changes (hair/nail/skin)
Please note:
Differential Diagnosis:
Treatment Approach:
Treatment should be started with all disciplines immediately. Pain is the leading symptom, which is associated with limb dysfunction and psychological distress. Patients with persistent pain demonstrate psychological symptoms. The psychological symptoms include depression and anxiety that are link with sleep loss. An interdisciplinary treatment approach is recommended, designed to the individual. The primary aims are to reduce pain, preserve or restore function, enable patient to manage their condition, and improve quality of life. Additionally, within the interdisciplinary approach, patients must receive the “four pillars of care”, which include education, pain relief, physical rehabilitation, and psychological interventions.
Medical Management:
Physical Therapy Implications:
Physical therapy is shown to be most effective in reducing pain and increasing function in the first year of CRPS, however, changes can still be made later than one year. It is important to provide the individual with an individualized program that address their impairments and symptoms. Possible interventions that have shown effectiveness in the literature could include:
Psychological Intervention: Psychological intervention can be helpful to reduce distress. They can also be helpful in identifying any psychological factors contributing to pain and disability. They can identify, explore, and address internal factors (e.g., counter-productive behavior patterns) or external influences (e.g., perverse incentives and family dynamics), which may perpetuate disability and dependency. Lastly, they can provide a practical problem-solving, goal-oriented approach involving both the patient and family to reduce barriers and promote health functioning.
Prognosis: Eighty-five percent of cases of CRPS improve or resolve within 18 months. Half of these cases continue with long-term functional problems and nearly half of patients do not return to work as a result of their chronic functional disability and residual pain.
Features of CRPS:
- Pain disproportionate to that expected after the relevant trauma, surgery, or immobilization
- Abnormal swelling
- Abnormal color (may appear red, mottled or cyanosed, or all at different times)
- Abnormal temperature
- Abnormal sweating
- Motor dysfunction
- Abnormal skin or nail appearance
Diagnostic Criteria: The diagnosis of CRPS is based on clinical examination and is given when patients meet the Budapest diagnostic criteria.
Budapest diagnostic criteria:
A) The patient has continuing pain which is disproportionate to any inciting event
B) The patient has at least one sign in tow or more of the categories
C) The patient reports at least one symptoms in three or more of the categories
D) No other diagnosis can be explain the signs and symptoms
Category
1. Sensory: Patients have signs and symptoms of Allodynia (to light touch and/or temperature sensation and/or deep somatic pressure and/or joint movement) and/or Hyperalgesia (to pinprick)
2. Vasomotor: Patients have signs and symptoms of temperature asymmetry (>1 degree Celsius) and/or skin color changes and/or skin color asymmetry.
3. Sudomotor/Edema: Patients have signs and symptoms of Oedema and/or sweating changes and/or swelling asymmetry
4. Motor/trophic: Patients have signs and symptoms of decreased range of motion and/or motor dysfunction (weakness, tremor, dystonia), and/or trophic changes (hair/nail/skin)
Please note:
- There is no distinction between treatment of type 1 or type 2. However, CRPS type 2 often requires a surgical intervention to fix the nerve lesion.
- If the patient has a lower number of signs and symptoms, or no signs, but signs and/or symptoms cannot be explained by another diagnosis, CRPS-NOS (not otherwise specified), can be diagnosed. Includes patients who had documented CRPS signs/symptoms in the past.
- If A, B, C, and D above are all ticked, please diagnosis CRPS.
Differential Diagnosis:
- Infection (bone, soft tissue, joint or skin)
- Orthopedic mal-fixation
- Joint instability
- Arthritis or arthorosis
- Bone or soft tissue injury (including stress fracture, instability or ligament damage)
- Compartment syndrome
- Neural injury (peripheral nerve damage, including compression or entrapment neuropathy, or central nervous system or spinal lesions)
- Thoracic outlet syndrome (due to nerve or vascular compression)
- Arterial insufficiency (usually after preceding trauma, atherosclerosis in the elderly or thorbangitis obliterans (Burger’s disease)
- Lymphatic or venous obstruction
- Gardner-Diamond Syndrome
- Brachial neuritis or plexitis (Parsonage-Turner syndrome or neuralgic amyotrophy)
- Erythromelalgia (may include all limbs)
- Self-harm
Treatment Approach:
Treatment should be started with all disciplines immediately. Pain is the leading symptom, which is associated with limb dysfunction and psychological distress. Patients with persistent pain demonstrate psychological symptoms. The psychological symptoms include depression and anxiety that are link with sleep loss. An interdisciplinary treatment approach is recommended, designed to the individual. The primary aims are to reduce pain, preserve or restore function, enable patient to manage their condition, and improve quality of life. Additionally, within the interdisciplinary approach, patients must receive the “four pillars of care”, which include education, pain relief, physical rehabilitation, and psychological interventions.
Medical Management:
- Drug therapy to reduce pain has strong evidence in the literature
- Procedures to reduce pain such as spinal cord stimulation and transcranial magnetic stimulation have limited evidence in the literature.
Physical Therapy Implications:
Physical therapy is shown to be most effective in reducing pain and increasing function in the first year of CRPS, however, changes can still be made later than one year. It is important to provide the individual with an individualized program that address their impairments and symptoms. Possible interventions that have shown effectiveness in the literature could include:
- Patient education and support
- Postural control
- Desensitization
- General exercises and strengthening
- Functional activities
- Mirror visual feedback
- Gait re-education
- TENS
- Relaxation techniques
- Facilitating self-management of condition
- Splinting
- Aquatic therapy
Psychological Intervention: Psychological intervention can be helpful to reduce distress. They can also be helpful in identifying any psychological factors contributing to pain and disability. They can identify, explore, and address internal factors (e.g., counter-productive behavior patterns) or external influences (e.g., perverse incentives and family dynamics), which may perpetuate disability and dependency. Lastly, they can provide a practical problem-solving, goal-oriented approach involving both the patient and family to reduce barriers and promote health functioning.
Prognosis: Eighty-five percent of cases of CRPS improve or resolve within 18 months. Half of these cases continue with long-term functional problems and nearly half of patients do not return to work as a result of their chronic functional disability and residual pain.
CRPS References
Cossins, L., Okel, RW., Cameron, H., Simpson, B., Poole, HM., & Goebel, A. (2012). Treatment of complex regional pain syndrome in adults: a systematic review of randomized controlled trials published from June 2000 to February 2012. Eur J Pain. (2):158-73. doi: 10.1002/j.1532-2149.2012.00217.x.
Freedman, M., Greis, AC., Marino, L., Sinha, AN., & Henstenburg, J. (2014). Complex Regional Pain Syndrome: Diagnosis and Treatment. Phys Med Rehabil Clin N Am. (2):291-303. doi: 10.1016/j.pmr.2014.01.003.
Goebel A, Barker CH, Turner-Stokes L et al . 2012. Complex regional pain syndrome in adults: UK guidelines for diagnosis, referral and management in primary and secondary care . London: Royal College of Physicians (RCP).
Freedman, M., Greis, AC., Marino, L., Sinha, AN., & Henstenburg, J. (2014). Complex Regional Pain Syndrome: Diagnosis and Treatment. Phys Med Rehabil Clin N Am. (2):291-303. doi: 10.1016/j.pmr.2014.01.003.
Goebel A, Barker CH, Turner-Stokes L et al . 2012. Complex regional pain syndrome in adults: UK guidelines for diagnosis, referral and management in primary and secondary care . London: Royal College of Physicians (RCP).
Suprascapular Nerve Pathology
Description: Suprascapular neuropathy is a rare diagnosis, however, its prevalence is increasing, so we must keep it on our radar as a cause of shoulder pain. The unique anatomy of suprascapular nerve makes it vulnerable to dynamic and static compression and injury.
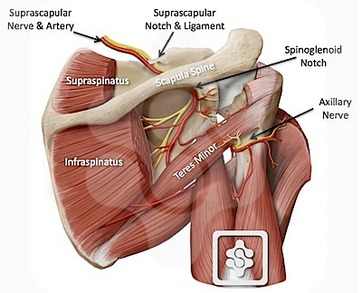
Anatomy: The suprascapular nerve complex arises from the upper trunk of the brachial plexus and receives contributions from the fifth and sixth cervical nerve roots and variable contributions from the 4th. Once the suprascapular nerve leaves the brachial plexus, it runs laterally through the posterior cervical triangle, posterior to the clavicle, and then across the superior border of the scapula and into the suprascapular notch. The suprascapular notch is a bony depression bordered by the base of the coracoid process laterally and the transverse scapular ligament superiorly. The suprascapular nerve is the only structure that passes through the transverse scapular ligament, which is known to ossify or hypertrophy causing stenosis of the notch and compression of the nerve. Furthermore, the suprascapular nerve passes from the suprascapular notch to the spinoglenoid notch, which is another location for possible pathology of the nerve. Lastly, it runs posterolateral through the supraspinatus fossa, supplying motor branches to the supraspinatus and infraspinatus.
Incidence: The incidence and prevalence of suprascapular neuropathy remain unknown. However, most reports deal with high-level overhead athletes, and the prevalence of suprascapular neuropathy in professional male volleyball players has ranged widely from 12.5% to 33%. The incidence and prevalence of the connection between suprascapular neuropathy and massive rotator cuff tears has been reported at 8%.
Mechanism of Injury: Irregular local anatomy, such as abnormally narrowing of the suprascapular and spinoglenoid notch, or a pathologic transverse scapular or spinoglenoid ligament, space-occupying lesions, massive rotator cuff tears, and dynamic repetitive microtrauma are all factors contributing to compression or tension on the suprascapular nerve that leads to nerve injury and symptoms.
Signs and Symptoms: Patients report a history that is not different from other common conditions around the shoulder. They will report a deep, dull, and chronic pain, localizing it to the superior, posterior, and lateral aspects of the shoulder with occasional radiation to their neck or lateral arm. Patients that are involved in throwing will describe a dull ache in the posterolateral corner of the spine of the scapula, exacerbated with throwing activities. Additionally, they will report subjective symptoms, which include weakness and fatigue with overhead activities. The pain typically worsens by arm positions involving horizontal adduction and internal rotation. When the suprascapular nerve is compressed, there is a potential for a 75% loss of abduction and external rotation strength.
Diagnosis: As we can see, it is difficult to diagnosis a suprascapular neuropathy from the history and physical examination alone since this condition often mimics conditions of the shoulder like rotator cuff pathologies. Suprascapular neuropathy affects the younger patients. As a result, this diagnosis must be considered in younger patients involved in overhead activities such as volleyball, baseball, tennis, basketball, and swimming. Additionally, given the connection of suprascapular neuropathy and rotator cuff tears, the diagnosis should be considered in any patient with a history of rotator cuff tear or a failed rotator cuff tear. A diagnosis must include imaging (radiographs, CT scan, or MRI). The gold standard for suprascapular neuropathy diagnostic testing is electromyography (EMG) and nerve conduction velocity (NCV) studies. Consequently, a diagnosis must include history, signs/symptoms, diagnostic conduction tests, and imaging.
Differential Diagnosis:
Examination: a comprehensive physical examination must be performed
Conservative Treatment: Suprascapular neuropathy, in the absence of space occupying lesions, is best treated with nonoperative measures due to the positive outcomes based on the current literature. A non-operative treatment approach consists of non-steroidal anti-inflammatory medications, avoidance of overhead activities, activity modification, and a physical therapy program emphasizing shoulder motion, rotator cuff, deltoid, and peri-scapular (shoulder) strengthening combined with scapular stabilization and mechanics exercises.
Operative Treatment: Some studies recommend early surgical decompression to avoid irreversible nerve damage and muscle atrophy. However, the indications for surgery are failed conservative treatment approaches, symptomatic condition (progressive pain and/or weakness), or lesion causing compression on the suprascapular nerve. The two methods that are used to decompress the nerve at the location of compression are indirect and direct methods.
Anatomy: The suprascapular nerve complex arises from the upper trunk of the brachial plexus and receives contributions from the fifth and sixth cervical nerve roots and variable contributions from the 4th. Once the suprascapular nerve leaves the brachial plexus, it runs laterally through the posterior cervical triangle, posterior to the clavicle, and then across the superior border of the scapula and into the suprascapular notch. The suprascapular notch is a bony depression bordered by the base of the coracoid process laterally and the transverse scapular ligament superiorly. The suprascapular nerve is the only structure that passes through the transverse scapular ligament, which is known to ossify or hypertrophy causing stenosis of the notch and compression of the nerve. Furthermore, the suprascapular nerve passes from the suprascapular notch to the spinoglenoid notch, which is another location for possible pathology of the nerve. Lastly, it runs posterolateral through the supraspinatus fossa, supplying motor branches to the supraspinatus and infraspinatus.
Incidence: The incidence and prevalence of suprascapular neuropathy remain unknown. However, most reports deal with high-level overhead athletes, and the prevalence of suprascapular neuropathy in professional male volleyball players has ranged widely from 12.5% to 33%. The incidence and prevalence of the connection between suprascapular neuropathy and massive rotator cuff tears has been reported at 8%.
Mechanism of Injury: Irregular local anatomy, such as abnormally narrowing of the suprascapular and spinoglenoid notch, or a pathologic transverse scapular or spinoglenoid ligament, space-occupying lesions, massive rotator cuff tears, and dynamic repetitive microtrauma are all factors contributing to compression or tension on the suprascapular nerve that leads to nerve injury and symptoms.
Signs and Symptoms: Patients report a history that is not different from other common conditions around the shoulder. They will report a deep, dull, and chronic pain, localizing it to the superior, posterior, and lateral aspects of the shoulder with occasional radiation to their neck or lateral arm. Patients that are involved in throwing will describe a dull ache in the posterolateral corner of the spine of the scapula, exacerbated with throwing activities. Additionally, they will report subjective symptoms, which include weakness and fatigue with overhead activities. The pain typically worsens by arm positions involving horizontal adduction and internal rotation. When the suprascapular nerve is compressed, there is a potential for a 75% loss of abduction and external rotation strength.
Diagnosis: As we can see, it is difficult to diagnosis a suprascapular neuropathy from the history and physical examination alone since this condition often mimics conditions of the shoulder like rotator cuff pathologies. Suprascapular neuropathy affects the younger patients. As a result, this diagnosis must be considered in younger patients involved in overhead activities such as volleyball, baseball, tennis, basketball, and swimming. Additionally, given the connection of suprascapular neuropathy and rotator cuff tears, the diagnosis should be considered in any patient with a history of rotator cuff tear or a failed rotator cuff tear. A diagnosis must include imaging (radiographs, CT scan, or MRI). The gold standard for suprascapular neuropathy diagnostic testing is electromyography (EMG) and nerve conduction velocity (NCV) studies. Consequently, a diagnosis must include history, signs/symptoms, diagnostic conduction tests, and imaging.
Differential Diagnosis:
- Parsonage-Turner Syndrome
- Acromioclavicular injury
- Labral tears
- Rotator cuff tears
- Cervical radiculopathy, nerve root injury, spondylosis
- Subacromial impingement
- Osteoarthritis
- Rheumatoid arthritis
- Axillary & subscapular impingement
- Shoulder instability
- Thoracic outlet syndrome
Examination: a comprehensive physical examination must be performed
- Inspect both shoulders and neck area for signs and symptoms of prior surgery or recent trauma
- Inspect evidence of atrophy on both shoulders and neck area specifically infraspinatus and supraspinatus
- Shoulder range of motion, strength, stability, and performance on specific tests
- Comprehensive neurological examination to rule out cervical radiculopathy and brachial plexus.
Conservative Treatment: Suprascapular neuropathy, in the absence of space occupying lesions, is best treated with nonoperative measures due to the positive outcomes based on the current literature. A non-operative treatment approach consists of non-steroidal anti-inflammatory medications, avoidance of overhead activities, activity modification, and a physical therapy program emphasizing shoulder motion, rotator cuff, deltoid, and peri-scapular (shoulder) strengthening combined with scapular stabilization and mechanics exercises.
Operative Treatment: Some studies recommend early surgical decompression to avoid irreversible nerve damage and muscle atrophy. However, the indications for surgery are failed conservative treatment approaches, symptomatic condition (progressive pain and/or weakness), or lesion causing compression on the suprascapular nerve. The two methods that are used to decompress the nerve at the location of compression are indirect and direct methods.
Suprascapular Nerve Pathology References
Blum A, Lecocq S, Louis M, Wassel J, Moisei A, & Teixeira P.2013. The Nerves Around the Shoulder. Eur J Radiol. 82(1):2-16. doi: 10.1016/j.ejrad.2011.04.033.
Budzik, JF., Wavreille, G., Pansini, V., Moraux, A., Demondion, X., & Cotton, A. (2012). Entrapment Neuropathies of the Shoulder. Magn Reson Imaging Clin N Am 20, 373-393. Doi:10.1016/j.mric.2012.01.013
Moen, T. C. et al. (2012). Suprascapular neuropathy: what does the literature show. Journal of Shoulder and Elbow Surgery, 21, 835-846.
Robert E. Boykin, MD; Darren J. Friedman, MD; Laurence D. Higgins, MD; Jon J.P. Warner, MD. (2010). J Bone Joint Surg Am, 92(13):2348-2364. http://dx.doi.org/10.2106/JBJS.I.01743.
Budzik, JF., Wavreille, G., Pansini, V., Moraux, A., Demondion, X., & Cotton, A. (2012). Entrapment Neuropathies of the Shoulder. Magn Reson Imaging Clin N Am 20, 373-393. Doi:10.1016/j.mric.2012.01.013
Moen, T. C. et al. (2012). Suprascapular neuropathy: what does the literature show. Journal of Shoulder and Elbow Surgery, 21, 835-846.
Robert E. Boykin, MD; Darren J. Friedman, MD; Laurence D. Higgins, MD; Jon J.P. Warner, MD. (2010). J Bone Joint Surg Am, 92(13):2348-2364. http://dx.doi.org/10.2106/JBJS.I.01743.
Long Thoracic Nerve Pathology
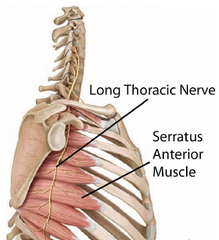
Anatomy: The long thoracic nerve arises from C5-C7. The C5 to C6 nerve roots pass through or on the scalenus medius muscle, whereas the C7 nerve passes between the anterior and middle scalene muscles. The C5 and C6 nerves unite with the C7 nerve distal to the scalene muscles to form the long thoracic nerve. (Safran, 2004)
Pathology: Repetition microtrauma in athletes, especially involved with stretching the nerve with activities like throwing objects with head rotated and laterally tilted away from affected extremity.
Nontraumatic issues could also cause problem such as bursa or scalene tightness.
Patient Presentation: Athletes with a long thoracic nerve injury will usually complain of pain or discomfort about the shoulder, neck, and/or scapular area, which is exacerbated by activity and/or by tilting their head away from and elevating the affected arm.
Patients will often have decreased active forward elevation and loss of power/strength of the shoulder. On examination from behind, the subject will have winging, especially at the inferior border, activities like pushing against the wall make abnormal position more clear. The subject may also have discoordinated scapulohumeral rhythm. In a thin or muscular subject, there may be wasting or atrophy of the serratus anterior.
Differential Diagnosis: Screening for long thoracic nerve injury includes ruling out cervical disk disease, brachial plexitis (Parsonage-Turner syndrome), rotator cuff tendinitis or tear, adhesive capsulitis, degenerative arthritis of the glenohumeral joint, degenerative arthritis of the acromioclavicular joint, glenohumeral instability, and TOS.
Prognosis: A traumatic long thoracic nerve palsy may resolve on its own within 1 year. However, cases due to Brachial Plexitis may take as long as 2 to 3 years to resolve. It has been reported that nonoperative treatment will not be successful in approximately one quarter of patients affected by long thoracic nerve injury. If symptoms do not resolve surgery is recommended.
Pathology: Repetition microtrauma in athletes, especially involved with stretching the nerve with activities like throwing objects with head rotated and laterally tilted away from affected extremity.
Nontraumatic issues could also cause problem such as bursa or scalene tightness.
Patient Presentation: Athletes with a long thoracic nerve injury will usually complain of pain or discomfort about the shoulder, neck, and/or scapular area, which is exacerbated by activity and/or by tilting their head away from and elevating the affected arm.
Patients will often have decreased active forward elevation and loss of power/strength of the shoulder. On examination from behind, the subject will have winging, especially at the inferior border, activities like pushing against the wall make abnormal position more clear. The subject may also have discoordinated scapulohumeral rhythm. In a thin or muscular subject, there may be wasting or atrophy of the serratus anterior.
Differential Diagnosis: Screening for long thoracic nerve injury includes ruling out cervical disk disease, brachial plexitis (Parsonage-Turner syndrome), rotator cuff tendinitis or tear, adhesive capsulitis, degenerative arthritis of the glenohumeral joint, degenerative arthritis of the acromioclavicular joint, glenohumeral instability, and TOS.
Prognosis: A traumatic long thoracic nerve palsy may resolve on its own within 1 year. However, cases due to Brachial Plexitis may take as long as 2 to 3 years to resolve. It has been reported that nonoperative treatment will not be successful in approximately one quarter of patients affected by long thoracic nerve injury. If symptoms do not resolve surgery is recommended.
Long Thoracic Nerve Pathology References
Safran M. Nerve Injury About the Shoulder in Athletes, Part 2: Long Thoracic Nerve, Spinal Accessory Nerve, Burners/Stingers, Thoracic Outlet Syndrome. American Journal Of Sports Medicine [serial online]. June 2004;32(4):1063-1076. Available from: Health Business Elite, Ipswich, MA. Accessed June 25, 2014.
A.T. Still University
Class of 2015
Published 07/03/2014
Class of 2015
Published 07/03/2014
