Musculoskeletal Conditions
Acromiocalvicular Osteoarthritis
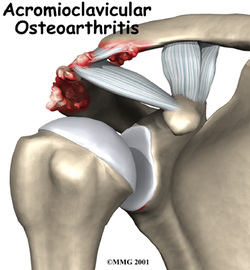
Osteoarthritis of the acromioclavicular (AC) joint is a result of high axial loads transferred through a small and incongruent joint surface during complex triplanar shoulder movements. While AC osteoarthritis (ACO) can occur in isolation it is commonly associated with rotator cuff disease; with or without the rotator cuff disease, ACO is likely to alter shoulder kinematics leading to compensatory movement, pain and functional loss. Identifying the kinematic impairments can provide a foundation for the therapist to base the intervention. Kinematic deviations are frequently occurring in the scapulothoracic region, primarily excessive internal rotation (protraction) during ascending and descending phase of abduction in the scapular plane. ACO pain may initially be isolated to the AC joint but it is often a generalized shoulder ache or impingement like pain description due to the poor kinematics of the scapula and scapulothoracic joint. Following a thorough history and examination kinematic deviations should be observed and addressed as early as possible to reduce pain and prevent further impairments. (Sousa et al., 2014)
AC Osteoarthritis Reference
Sousa Cde, O., Camargo, P. R., Ribeiro, I. L., Reiff, R. B., Michener, L. A., & Salvini, T. F. (2014). Motion of the shoulder complex in individuals with isolated acromioclavicular osteoarthritis and associated with rotator cuff dysfunction: Part 1 - Three-dimensional shoulder kinematics. J Electromyogr Kinesiol, 24(4), 520-530.
Snapping Scapula and Bursitis
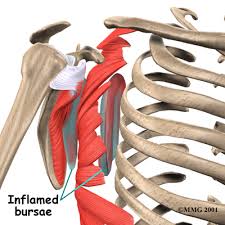
Etiology/History: Snapping scapula syndrome is caused by either osseous lesions or scapulothoracic bursitis. (Frank, 2013)
Scapulothoracic bursitis and snapping scapula are rare diagnoses associated with pain. It may or may not include mechanical crepitus. It's commonly found in young, active patients who perform repetitive overhead activities. It can result from anatomic scapular or thoracic variations, muscle abnormalities, and bony or soft-tissue masses. (Gaskill et al., 2013)
Patients have often experienced this for quite a long time. Symptoms range from mild, intermittent discomfort to notable functional disability. Patients may report decreased athletic performance, increased pain with overhead activities, audible or palpable crepitus. This can be due to trauma or overuse. Bursitis and scapular snapping can occur concomitantly but can occur independently, as well. (Gaskill et al., 2013)
Diagnosing: A firm knowledge and understanding of the periscapular anatomy is a must. A thorough history and physical examination must be performed and if it sounds like snapping scapula syndrome then imagining is usually done: plain radiography, computed tomography (CT), magnetic resonance imaging (MRI), and ultrasonography. (Frank et al., 2013)
The physical examination should begin by examining the cervical and thoracic spine for fixed or postural kyphosis which may contribute abnormal scapulothoracic movement. Referred pain to the scapulothoracic area can be due to cervical degeneration. Active and passive range of motion of the upper extremities should be tested, paying particular attention to the scapulothoracic motion. The therapist should check for crepitus in the scapulothoracic and glenohumeral joints during active and passive movement and examine dynamic movement of the scapula, looking for scapular winging, which may be due to motor dysfunction or masses in the scapulothoracic region. Be aware of pseudowinging which may occur because the patient is compensating for pain or has learned motion patterns to avoid crepitus. Other symptoms include tenderness and fullness of a bursa in the scapular region. Muscular strength should be tested, especially the trapezius, rhomboid, levator scapulae, serratus anterior, and lattisimus dorsi. (Gaskill et al., 2013)
Treatment: First-line of treatment for scapulothoracic bursitis is nonoperative: activity modification, analgesics, nonsteroidal anti-inflammatories, physical threapy for strengthening of the periscapular musculature and rotator cuff and improvement of scapular positioning. Nonoperative management is usually attempted for 6 months to a year before trying surgical management such as surgical bursectomy and or superomedial angle resection. (Frank et al., 2013)
Rehabilitation after surgery:
Scapulothoracic bursitis and snapping scapula are rare diagnoses associated with pain. It may or may not include mechanical crepitus. It's commonly found in young, active patients who perform repetitive overhead activities. It can result from anatomic scapular or thoracic variations, muscle abnormalities, and bony or soft-tissue masses. (Gaskill et al., 2013)
Patients have often experienced this for quite a long time. Symptoms range from mild, intermittent discomfort to notable functional disability. Patients may report decreased athletic performance, increased pain with overhead activities, audible or palpable crepitus. This can be due to trauma or overuse. Bursitis and scapular snapping can occur concomitantly but can occur independently, as well. (Gaskill et al., 2013)
Diagnosing: A firm knowledge and understanding of the periscapular anatomy is a must. A thorough history and physical examination must be performed and if it sounds like snapping scapula syndrome then imagining is usually done: plain radiography, computed tomography (CT), magnetic resonance imaging (MRI), and ultrasonography. (Frank et al., 2013)
The physical examination should begin by examining the cervical and thoracic spine for fixed or postural kyphosis which may contribute abnormal scapulothoracic movement. Referred pain to the scapulothoracic area can be due to cervical degeneration. Active and passive range of motion of the upper extremities should be tested, paying particular attention to the scapulothoracic motion. The therapist should check for crepitus in the scapulothoracic and glenohumeral joints during active and passive movement and examine dynamic movement of the scapula, looking for scapular winging, which may be due to motor dysfunction or masses in the scapulothoracic region. Be aware of pseudowinging which may occur because the patient is compensating for pain or has learned motion patterns to avoid crepitus. Other symptoms include tenderness and fullness of a bursa in the scapular region. Muscular strength should be tested, especially the trapezius, rhomboid, levator scapulae, serratus anterior, and lattisimus dorsi. (Gaskill et al., 2013)
Treatment: First-line of treatment for scapulothoracic bursitis is nonoperative: activity modification, analgesics, nonsteroidal anti-inflammatories, physical threapy for strengthening of the periscapular musculature and rotator cuff and improvement of scapular positioning. Nonoperative management is usually attempted for 6 months to a year before trying surgical management such as surgical bursectomy and or superomedial angle resection. (Frank et al., 2013)
Rehabilitation after surgery:
- Open technique: Typically the shoulder is immobilized in a sling for up to 4 weeks postoperatively to facilitate muscle healing. Pendulum and PROM exercises begin shortly after surgery. AROM typically starts around 8 weeks postop. Strengthening exercises start around 12 weeks.
- Arthroscopic: A sling is used only for about a week for comfort. PROM and pendulum exercises are begun immediately. Progression to AROM and strengthening is based on patient tolerance. (Gaskill et al., 2013)
Snapping Scapula and Bursitis References***
Frank, R. M., Ramirez, J., Chalmers, P. N., McCormick, F. M., & Romeo, A. A. (2013). Anatomy and Snapping Scapula Syndrome. Anatomy Research International, 2013, 1-9.
Gaskill, T., & Millett, P. J. (2013). Snapping Scapula Syndrome: Diagnosis and Management. Journal of the American Academy of Orthopaedic Surgeons, 21(4), 214-224.
***These references are review articles.
Gaskill, T., & Millett, P. J. (2013). Snapping Scapula Syndrome: Diagnosis and Management. Journal of the American Academy of Orthopaedic Surgeons, 21(4), 214-224.
***These references are review articles.
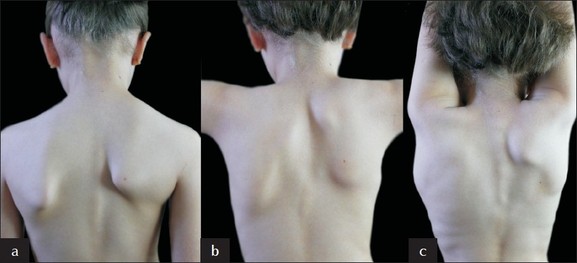
Sprengel’s Deformity

Demographics: Equal among males and females
Anatomy: Rare shoulder deformity associated with scoliosis, vertebral, and rib deformities, spina bifida, abnormal muscular torticollis. It is described as undescended scapula. It is elevated and adducted with dysplastic qualities.
The Cavendish Classification
The Rigault Classification
Treatments: Can be treated with surgery if it interferes with function, or patient worries too much about physical appearance. The surgeries that can be done are Green’s procedure, Woodward’s procedure, and Scapular Osteotomy. Each surgery carries with it different risk factors. Green’s procedure and Woodward’s procedure could compromise the brachial plexus, or cause scapular winging. Green’s procedure and Scapular Osteotomy can lead to hypertrophy of the scar tissue.
PT implications: PT’s should educate their patient about the options for treatment, and encourage the patient to ask the doctor about side-effects of surgery. After surgery, PT’s need to look for scapular winging, and treat accordingly.
After Green’s procedure the recommended treatment is cautious shoulder immobilization for 4 weeks. Woodward’s procedure describes waiting only for the wounds to heal before active rehabilitation. The Edinburgh group calls for accelerated rehabilitation following their scapular osteotomy, but full active rehabilitation could be delayed for 6 weeks.
Anatomy: Rare shoulder deformity associated with scoliosis, vertebral, and rib deformities, spina bifida, abnormal muscular torticollis. It is described as undescended scapula. It is elevated and adducted with dysplastic qualities.
The Cavendish Classification
- Very mild, shoulder level and deformity invisible when dressed
- Mild, shoulders almost level, lump visible in web of the neck when dressed
- Moderate, shoulder elevated 2–5 cm. Deformity easily visible
- Severe, superior angle of scapula near occiput, with or without neck webbing
The Rigault Classification
- Supero-medial angle lower than T2 but above T4 transverse process
- Supero-medial angle located between C5 and T2 transverse process
- Supero-medial angle above C5 transverse process
Treatments: Can be treated with surgery if it interferes with function, or patient worries too much about physical appearance. The surgeries that can be done are Green’s procedure, Woodward’s procedure, and Scapular Osteotomy. Each surgery carries with it different risk factors. Green’s procedure and Woodward’s procedure could compromise the brachial plexus, or cause scapular winging. Green’s procedure and Scapular Osteotomy can lead to hypertrophy of the scar tissue.
PT implications: PT’s should educate their patient about the options for treatment, and encourage the patient to ask the doctor about side-effects of surgery. After surgery, PT’s need to look for scapular winging, and treat accordingly.
After Green’s procedure the recommended treatment is cautious shoulder immobilization for 4 weeks. Woodward’s procedure describes waiting only for the wounds to heal before active rehabilitation. The Edinburgh group calls for accelerated rehabilitation following their scapular osteotomy, but full active rehabilitation could be delayed for 6 weeks.
Sprengel’s Deformity Reference
Radmore L, Thomas W, Tasker A, Diamond D, Amirfeyz R, Gargan M. Syndrome: Sprengel’s deformity. Orthopaedics And Trauma [serial online]. January 1, 2011;25:131-134. Available from: ScienceDirect, Ipswich, MA. Accessed June 25, 2014
Latissimus Dorsi Stiffness
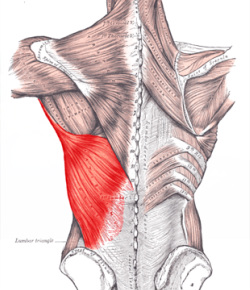
Latissimus dorsi stiffness could lead to increased dyskinesia. Laudner et al. found that latissimus dorsi stiffness showed moderate-to-good relationships with increased scapular upward rotation ( r > −0.63, P < 0.002) and posterior tilt ( r > −0.62, P < 0.004) at all four angles of humeral elevation. Increased latissimus dorsi stiffness also showed moderate-to-good relationships with decreased scapular internal rotation at humeral elevation angles of 60° ( r = 0.47, P = 0.03) and 90° ( r = 0.54, P = 0.01). Only scapular internal rotation at 30° ( r = 0.18, P = 0.24) and 110° ( r = 0.28, P = 0.13) of humeral elevation showed little-to-no relationship with latissimus dorsi stiffness.
The study measured dyskinesia by placing three electromagnetic receivers on various anatomical positions. They then tested latissimus dorsi stiffness by having the patient placed in a prone position with their dominant arm resting by their head in a flexed position. The investigator placed the probe of the myotonometer approximately 5 cm inferior to the inferior scapular border. The myotonometer was compressed a total of 8 times perpendicularly into the muscle until the myotonometer software indicated reaching the specified target force increments (0.25–2.0 kg). Muscle stiffness was defined as the amount of tissue displacement in response to the applied force.
PT implications: If a patient presents with scapular dyskinesia it may be necessary to test all muscle lengths. While this study shows a possible link with latissimus dorsi stiffness, other impairments may be indicated like tight pectoralis minor, pectoralis major, and tight trapezius.
Possible biomechanic problems relating to tight latissimus dorsi:
Laudner et al. proposed in their study that as subjects elevated their humerus during the scapular assessment task, a stiff latissimus dorsi, which inserts onto the humerus, may have pulled the inferior scapular border superiorly and laterally resulting in increased upward rotation. Similarly, a stiff latissimus dorsi could potentially place increased pressure on the inferior scapular border moving it anteriorly towards the thorax resulting in increased posterior tilt. Lastly, a stiff latissimus dorsi may result in an increased pull on the scapula in the direction of external rotation as the lower fibers run towards their origin at the ilium, lower vertebra and posterior ribs.
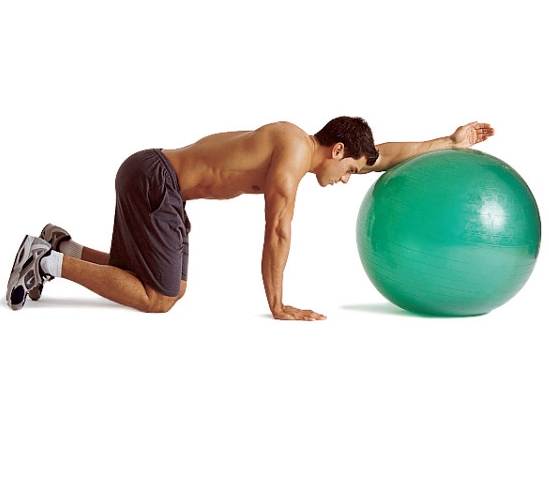
Treatments: If the latissimus dorsi is tight an effective treatment is to stretch the latissimus dorsi on an exercise ball. (See image below) When stretching the latissimus dorsi make sure your cervical spine is in a neutral position.
Hrysomallis et al. found that stretching anterior chest wall, and strengthening scapular retractors can correct scapular position.
The study measured dyskinesia by placing three electromagnetic receivers on various anatomical positions. They then tested latissimus dorsi stiffness by having the patient placed in a prone position with their dominant arm resting by their head in a flexed position. The investigator placed the probe of the myotonometer approximately 5 cm inferior to the inferior scapular border. The myotonometer was compressed a total of 8 times perpendicularly into the muscle until the myotonometer software indicated reaching the specified target force increments (0.25–2.0 kg). Muscle stiffness was defined as the amount of tissue displacement in response to the applied force.
PT implications: If a patient presents with scapular dyskinesia it may be necessary to test all muscle lengths. While this study shows a possible link with latissimus dorsi stiffness, other impairments may be indicated like tight pectoralis minor, pectoralis major, and tight trapezius.
Possible biomechanic problems relating to tight latissimus dorsi:
Laudner et al. proposed in their study that as subjects elevated their humerus during the scapular assessment task, a stiff latissimus dorsi, which inserts onto the humerus, may have pulled the inferior scapular border superiorly and laterally resulting in increased upward rotation. Similarly, a stiff latissimus dorsi could potentially place increased pressure on the inferior scapular border moving it anteriorly towards the thorax resulting in increased posterior tilt. Lastly, a stiff latissimus dorsi may result in an increased pull on the scapula in the direction of external rotation as the lower fibers run towards their origin at the ilium, lower vertebra and posterior ribs.
Treatments: If the latissimus dorsi is tight an effective treatment is to stretch the latissimus dorsi on an exercise ball. (See image below) When stretching the latissimus dorsi make sure your cervical spine is in a neutral position.
Hrysomallis et al. found that stretching anterior chest wall, and strengthening scapular retractors can correct scapular position.

Latissimus Dorsi Stiffness References
Hrysomallis C. Effectiveness of strengthening and stretching exercises for the postural correction of abducted scapulae: a review. Journal Of Strength And Conditioning Research / National Strength & Conditioning Association [serial online]. February 2010;24(2):567-574. Available from: MEDLINE, Ipswich, MA. Accessed June 30, 2014
Laudner K, Williams J. Original research: The relationship between latissimus dorsi stiffness and altered scapular kinematics among asymptomatic collegiate swimmers. Physical Therapy In Sport [serial online]. February 1, 2013;14:50-53. Available from: ScienceDirect, Ipswich, MA. Accessed June 26, 2014.
Laudner K, Williams J. Original research: The relationship between latissimus dorsi stiffness and altered scapular kinematics among asymptomatic collegiate swimmers. Physical Therapy In Sport [serial online]. February 1, 2013;14:50-53. Available from: ScienceDirect, Ipswich, MA. Accessed June 26, 2014.
Kyphosis
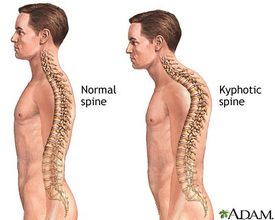
Excessive Thoracic Kyphosis is essentially a postural problem, but it can also manifest as a variety of other symptoms:
• pain
• limited function
• poor health and disease
• increased mental stress
Kyphosis can be idiopathic in nature, or can occur as a result of poor posture. Scheuermann disease and postural round back are often identified in adolescents. Congenital abnormalities, such as failure of formation or failure of segmentation of the spinal elements, can cause a pathologic kyphosis. Autoimmune arthropathy, such as ankylosing spondylitis, can cause rigid kyphosis as the disease progresses. Kyphosis can also develop as a result of trauma, a spinal tumor, or an infection. Known metabolic disorders and dwarfing conditions can lead to kyphosis. Patients with COPD tend to have a forward posture to help them with breathing. Changes in structure to the spine may be effected by patients continuously hyper-inflating their lungs which then may effect scapula movement causing pain. It is important for PT’s to recognize how changes in function relating to the scapula can occur.
Urbanowicz et al. found a greater upward rotation and scapular elevation, as well as lesser head protraction and anterior tilt of the scapula on the left side, exhibiting a statistically significant difference from the right side in the group of patients with COPD.
Treatment should be aimed at prevention.
• pain
• limited function
• poor health and disease
• increased mental stress
Kyphosis can be idiopathic in nature, or can occur as a result of poor posture. Scheuermann disease and postural round back are often identified in adolescents. Congenital abnormalities, such as failure of formation or failure of segmentation of the spinal elements, can cause a pathologic kyphosis. Autoimmune arthropathy, such as ankylosing spondylitis, can cause rigid kyphosis as the disease progresses. Kyphosis can also develop as a result of trauma, a spinal tumor, or an infection. Known metabolic disorders and dwarfing conditions can lead to kyphosis. Patients with COPD tend to have a forward posture to help them with breathing. Changes in structure to the spine may be effected by patients continuously hyper-inflating their lungs which then may effect scapula movement causing pain. It is important for PT’s to recognize how changes in function relating to the scapula can occur.
Urbanowicz et al. found a greater upward rotation and scapular elevation, as well as lesser head protraction and anterior tilt of the scapula on the left side, exhibiting a statistically significant difference from the right side in the group of patients with COPD.
Treatment should be aimed at prevention.
Kyphosis References
Cassidy R, Kyphosis, Medscape, updated Dec 10, 2013, Available from: http://emedicine.medscape.com/article/1264959-overview#a0102 Accessed June 27, 2014
Urbanowicz R, Lamb J, Todd I, Corne J, Fairclough L. Orientation and position of the scapula, head and kyphosis thoracic in male patients with COPD. Canadian Journal Of Respiratory Therapy [serial online]. July 2009;45(2):30-34. Available from: CINAHL, Ipswich, MA. Accessed June 26, 2014
Urbanowicz R, Lamb J, Todd I, Corne J, Fairclough L. Orientation and position of the scapula, head and kyphosis thoracic in male patients with COPD. Canadian Journal Of Respiratory Therapy [serial online]. July 2009;45(2):30-34. Available from: CINAHL, Ipswich, MA. Accessed June 26, 2014
A.T. Still University
Class of 2015
Published 07/03/2014
Class of 2015
Published 07/03/2014
